It has been a very busy week as tends to happen in November, as the hours of sunlight decline and the expectations at school increase.
So I will not add another chapter this week to my vision of the dance between genetics and environment and the origins of mental illness.
I hope I have engaged you in this dance, as it begins in the first years of life.
I hope I have brought a slightly different perspective of the context of mood states and the relational nature of our selves as we emerge from potential selves to actual selves.
My hope here is to break out of the dichotomy of genetic determinism and its opposite pole of environmental determinism. In breaking out of these two positions I hope to get away from the idea that mental illness needs to be blamed on individuals. Nuclear families (and sometimes single parents) have the burden of being the guardians of children's development on their shoulders in our modern world. Yet they cannot be expected to carry this burden alone. We must join them in taking responsibility for the environment of development as a society. Blaming parents for the ills of children is counterproductive and unfounded. Parents are usually doing their very best in difficult situations. I believe in shared responsibility, not blame. As mental health providers we can take our share of responsibility and empower others to take theirs, while facilitating access to the support that will make this possible.
The idea of genetic determinism is tempting as an ideology which absolves others of responsibility, but it is untenable. Genetic determinism also disempowers the individual and the family suggesting that genetics is destiny and that only perhaps genetic interventions or alternatively palliative psychopharmacology are options. These are false conclusions.
I hope you have a good November week.

Monday, 12 November 2012
Sunday, 4 November 2012
Coming Detached

Hospital Dramas
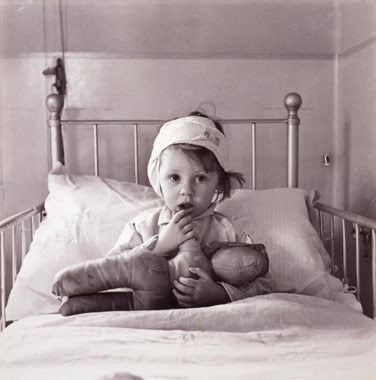
John Bowlby and his colleague James Robertson created a documentary in 1952 titled “A Two Year old goes to the Hospital”. This film depicted the series of stages a two year old underwent while hospitalized and separated from her parents. At the time it was hospital policy for children to be separated from parents while undergoing hospital treatments, with parents having as little as once a week contact with their hospitalized child. This was a practice that would change, in part due to this very documentary, as viewers of that time reacted with concern to the impact of such separations on very young children.
Stages of Detachment

In his seminal work, Bowlby explored attachment disruptions of various kinds and detailed children's emotional reactions to these disruptions. When attachments are threatened, children react at first with anxiety, a high energy state that promotes calling and clinging. When attachments are threatened further these reactions are often heighten into a stage he referred to as protest, which can include anger. Bowlby proposed that this high energy state might allow a child to overcome obstacles to reuniting with the attachment figure and communicate reproach in an effort to discourage the attachment figure from becoming unavailable in the future. If these efforts fail, the subsequent stage Bowlby described was the low energy state of despair, characterized by sadness, listlessness and resignation. One can see how this would also be an adaptive survival behavior for a child, conserving energy and avoiding danger when separated from a parent. This stage was followed by a stage Bowlby referred to as detachment. In this stage the child mobilizes energy, but attachment emotions are downplayed. Bowlby hypothesized that this was a defensive reaction, inhibiting unhelpul emotions in order to go about the necessary activities of survival. In hospital, the youngster would start to allow care from the nurses and engage in day to day activities. However when parents would return, children would ignore or avoid them. This detached reaction could go on for some time before the child would begin to demonstrate attachment emotions (including anger and clinging) towards the parent once again. Bowlby's stages may sound familiar, as they are related to the stages of grief and loss that we continue to manifest throughout adult life as we respond to threats or losses to our ongoing attachment relationships.
Unknown Unknowns
Here we see the full range of emotional reactions of fear, sadness, anger and numbness in the context of relational states. Very young children may manifest these emotional states in their efforts to reestablish or cope with threats to their key relationships. It is important here to understand that working models of attachment and their connections to emotional states are coded in implicit memory, in the early developing right hemisphere. Therefore the child, and later the adult, is often not aware of the reasons for their emotional reactions to these attachment cues. The older child, when asked why they are frightened or angry will often answer truthfully that they do not know why. At times they will attribute their fears to monsters rather than the loss of the attachment figure, or their anger may be directed at a target other than the attachment figure.
Modern Dramas

In our modern world we no longer separate children from their parents in hospitals. However our children do experience long periods of separation from parents. In overcrowded daycares and schools, often with both parents employed to meet the demands of modern expenses, very young children continue to experience threats to attachment. Parental isolation and depression can lead to parents being unavailable due to their own emotional states. Children frequently turn to other children for their attachment needs, a pattern that has become increasingly common as children can now contact one another easily with electronic devices. Although more common in adolescence, children can turn towards other children as their source of comfort and preferred source of positive attention. In this process they start to identify with peer values rather than adult values, much to their parents chagrin. Within these unstable relationships with peers, children can turn on one another or themselves in an effort to gain the acceptance and security that they crave. Parents can often feel helpless to reestablish these bonds once they have fractured despite their best intentions.
Chidren react, Parents react

As children react to perceived attachment threats with the range of emotional states that Bowlby first identified, these emotional reactions themselves can increase the challenges in these fragile relationships with parents. Fear and clinging can lead to parental frustration and resentment. Anger can result in defensive anger in parents. Sadness and withdrawal can be perceived as rejection by a sensitive parent or laziness. It is easy to see how emotional reactions can lead to cascading relationship breakdowns in fragile social situations. Unfortunately the remedies health care providers sometimes prescribe can contribute to the problem. These interventions can range from ill-advised exposure exercises in anxious children, to harsh time outs or punishments or cracking down with tough love on an unmotivated youngster. If we do not tune in to the need for restoring attachment relationships, these problems can often escalate. Healthy attachment relationships form the underpinnings of natural parental authority. In "Hold Onto Your Kids", Gordon Neufeld and Gabor Mate have argued persuasively for promoting parental attachment in a world where peer attachments can easily become all-consuming for young people. We should be careful to not inadvertently undermine our own role as parents by overdoing our promotion of peer activities and ourselves adding to the already existing pressure on youngster's to “fit in” with peers. It is time we developed a better understanding of the relational context of the mental health of our young people. Perhaps one day we will look back on the daycare and school environments we accept as ordinary today with as much disbelief as we do the hospital environments of 60 years ago.
Subscribe to:
Comments (Atom)