It has been a very busy week as tends to happen in November, as the hours of sunlight decline and the expectations at school increase.
So I will not add another chapter this week to my vision of the dance between genetics and environment and the origins of mental illness.
I hope I have engaged you in this dance, as it begins in the first years of life.
I hope I have brought a slightly different perspective of the context of mood states and the relational nature of our selves as we emerge from potential selves to actual selves.
My hope here is to break out of the dichotomy of genetic determinism and its opposite pole of environmental determinism. In breaking out of these two positions I hope to get away from the idea that mental illness needs to be blamed on individuals. Nuclear families (and sometimes single parents) have the burden of being the guardians of children's development on their shoulders in our modern world. Yet they cannot be expected to carry this burden alone. We must join them in taking responsibility for the environment of development as a society. Blaming parents for the ills of children is counterproductive and unfounded. Parents are usually doing their very best in difficult situations. I believe in shared responsibility, not blame. As mental health providers we can take our share of responsibility and empower others to take theirs, while facilitating access to the support that will make this possible.
The idea of genetic determinism is tempting as an ideology which absolves others of responsibility, but it is untenable. Genetic determinism also disempowers the individual and the family suggesting that genetics is destiny and that only perhaps genetic interventions or alternatively palliative psychopharmacology are options. These are false conclusions.
I hope you have a good November week.

Monday, 12 November 2012
Sunday, 4 November 2012
Coming Detached

Hospital Dramas
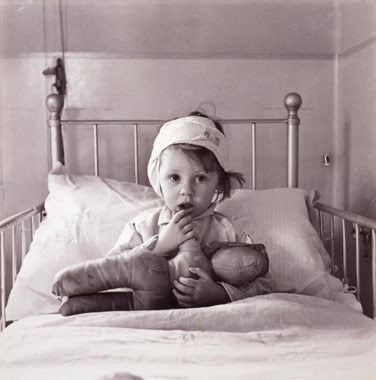
John Bowlby and his colleague James Robertson created a documentary in 1952 titled “A Two Year old goes to the Hospital”. This film depicted the series of stages a two year old underwent while hospitalized and separated from her parents. At the time it was hospital policy for children to be separated from parents while undergoing hospital treatments, with parents having as little as once a week contact with their hospitalized child. This was a practice that would change, in part due to this very documentary, as viewers of that time reacted with concern to the impact of such separations on very young children.
Stages of Detachment

In his seminal work, Bowlby explored attachment disruptions of various kinds and detailed children's emotional reactions to these disruptions. When attachments are threatened, children react at first with anxiety, a high energy state that promotes calling and clinging. When attachments are threatened further these reactions are often heighten into a stage he referred to as protest, which can include anger. Bowlby proposed that this high energy state might allow a child to overcome obstacles to reuniting with the attachment figure and communicate reproach in an effort to discourage the attachment figure from becoming unavailable in the future. If these efforts fail, the subsequent stage Bowlby described was the low energy state of despair, characterized by sadness, listlessness and resignation. One can see how this would also be an adaptive survival behavior for a child, conserving energy and avoiding danger when separated from a parent. This stage was followed by a stage Bowlby referred to as detachment. In this stage the child mobilizes energy, but attachment emotions are downplayed. Bowlby hypothesized that this was a defensive reaction, inhibiting unhelpul emotions in order to go about the necessary activities of survival. In hospital, the youngster would start to allow care from the nurses and engage in day to day activities. However when parents would return, children would ignore or avoid them. This detached reaction could go on for some time before the child would begin to demonstrate attachment emotions (including anger and clinging) towards the parent once again. Bowlby's stages may sound familiar, as they are related to the stages of grief and loss that we continue to manifest throughout adult life as we respond to threats or losses to our ongoing attachment relationships.
Unknown Unknowns
Here we see the full range of emotional reactions of fear, sadness, anger and numbness in the context of relational states. Very young children may manifest these emotional states in their efforts to reestablish or cope with threats to their key relationships. It is important here to understand that working models of attachment and their connections to emotional states are coded in implicit memory, in the early developing right hemisphere. Therefore the child, and later the adult, is often not aware of the reasons for their emotional reactions to these attachment cues. The older child, when asked why they are frightened or angry will often answer truthfully that they do not know why. At times they will attribute their fears to monsters rather than the loss of the attachment figure, or their anger may be directed at a target other than the attachment figure.
Modern Dramas

In our modern world we no longer separate children from their parents in hospitals. However our children do experience long periods of separation from parents. In overcrowded daycares and schools, often with both parents employed to meet the demands of modern expenses, very young children continue to experience threats to attachment. Parental isolation and depression can lead to parents being unavailable due to their own emotional states. Children frequently turn to other children for their attachment needs, a pattern that has become increasingly common as children can now contact one another easily with electronic devices. Although more common in adolescence, children can turn towards other children as their source of comfort and preferred source of positive attention. In this process they start to identify with peer values rather than adult values, much to their parents chagrin. Within these unstable relationships with peers, children can turn on one another or themselves in an effort to gain the acceptance and security that they crave. Parents can often feel helpless to reestablish these bonds once they have fractured despite their best intentions.
Chidren react, Parents react

As children react to perceived attachment threats with the range of emotional states that Bowlby first identified, these emotional reactions themselves can increase the challenges in these fragile relationships with parents. Fear and clinging can lead to parental frustration and resentment. Anger can result in defensive anger in parents. Sadness and withdrawal can be perceived as rejection by a sensitive parent or laziness. It is easy to see how emotional reactions can lead to cascading relationship breakdowns in fragile social situations. Unfortunately the remedies health care providers sometimes prescribe can contribute to the problem. These interventions can range from ill-advised exposure exercises in anxious children, to harsh time outs or punishments or cracking down with tough love on an unmotivated youngster. If we do not tune in to the need for restoring attachment relationships, these problems can often escalate. Healthy attachment relationships form the underpinnings of natural parental authority. In "Hold Onto Your Kids", Gordon Neufeld and Gabor Mate have argued persuasively for promoting parental attachment in a world where peer attachments can easily become all-consuming for young people. We should be careful to not inadvertently undermine our own role as parents by overdoing our promotion of peer activities and ourselves adding to the already existing pressure on youngster's to “fit in” with peers. It is time we developed a better understanding of the relational context of the mental health of our young people. Perhaps one day we will look back on the daycare and school environments we accept as ordinary today with as much disbelief as we do the hospital environments of 60 years ago.
Sunday, 28 October 2012
Getting Attached
Under stress are you cool as a cucumber or hot headed? Do you trust others to be available, or doubt them? Do you tend to withdraw from your partner when stressed or cling to them? Do you challenge authority and feel more comfortable when you are in charge, or do you hate to rock the boat? The early stages of development have a lot to do with the “working models” we use to decide on how to include others or not include them in our lives.
In the last two posts I discussed the process of attunement and sensory regulation that begins in the first nine months and the process of shame states and repair of the second nine months. When this process goes well it allows us to enjoy exploring our world and to respond appropriately to the needs of others. In this post I will discuss how we negotiate our needs with the caregivers in our world.
Finding Home Base

In this post, I want to discuss the concept of attachment, first identified by John Bowlby in the 1950s. Attachment is a relationship between an infant and its parent that evolves through the first year and a half of life. It is a process whereby an infant creates a “working model” to predict and direct the availability (that is the accessibility and responsiveness) of caregiving others in their world. In this process infants figure out in whose arms they will find comfort when it is needed and how to get it.
From the sixth week of life the infant can tell his caregivers apart and begins to respond unhappily when they are in the care of a stranger. Infants show preference for one caregiver who becomes the infants primary “attachment figure”. Human infants can allow (remember my earlier post "Mothers and Others") more than one attachment figure, but there remains a hierarchy of the most preferred attachment figure which the infant will select when available, and demand when most alarmed. Infants bond to their primary caregiver through the process of attunement, that is with a caregiver who is sensitive and responsive. The quality of this social engagement is more important than the amount of time spent with that caregiver.
Homing Beacon

The attachment system is a motivational system which leads the infant to seek out its caregiver for safety, security and protection when it is distressed. When the attachment system is aroused the infant is less able to calmly explore their surroundings. The infant will vocalize and call the caregiver and, when able, will move towards the caregiver. When they have safely been reunited with the caregiver, the distress resolves, the infant is comforted and they can resume exploration. The biological utility of this behaviour is clear. In the process of evolution, having a well-tuned attachment system maintains the safety and security of infants in an uncertain world. The neurobiology of this system is now well understood. A stressful situation activates the infants sympathetic nervous system (speeding up heart rate and mobilizing energy), the motivational system (involving the dopamine system) is now directed away from exploration and towards seeking out the caregiver When this is achieved the infant is soothed and comforted (a process involving oxytocin, serotonin and endorphins). When this behaviour pattern works, it is reinforced. If it is not successful, other patterns of behaviour emerge.
The Strange Situation

Mary Ainsworth, a colleague of Bowlby, was a pioneer in studying toddlers’ attachment behaviour. She set up a series of laboratory scenarios that would mildly stress toddlers and observed how they responded. She identified three patterns of attachment. Further work by Margaret Main added a fourth pattern.
Ainsworth separated attachment styles into secure and insecure. The most famous observation scenario she created to rate children was called the “Strange Situation”. In this scenario the parent and the toddler are in a room, and are joined by a non-threatening stranger. At a prearranged point the parent leaves the room unannounced. After a few minutes, the parent returns.
Secure or Insecure
Securely attached toddlers were seen to protest (cry and call) when the parent left, but were able to calm quickly when the parent returned and comforted them. Ainsworth also identified two patterns that she referred to as insecure attachment.
In the first, the child does not protest when the parent departs and when the parent returns the child ignores, avoids the parent, or approaches very hesitantly. Despite not protesting, the child’s exploration of the toys deteriorated and later studies revealed that these infants are showing stress reactions (elevated heart rates etc.) during the departure even though they are not protesting. This pattern was termed an avoidant attachment .
In the second pattern, the child does protests, often in a dramatic fashion, sometimes clinging tightly to the departing parent. When the parent returns the infant continues to protest, even directing aggression toward the parent and does not settle for some time. This second “insecure” pattern was referred to as an ambivalent attachment.
Mary Main demonstrated a fourth pattern, which she referred to as an insecure disorganized attachment. These infants appeared to be confused as to how to respond. The child might protest and then withdraw or appear frozen in indecision. This pattern has been demonstrated to occur in the most troubled of parent child situations and has been related to the worst outcomes. None of these patterns is in itself a “disorder”. They are merely relationship patterns. They have also been shown to have remarkable staying power although they can change as development progresses. These pattern have been shown to persist into adulthood in our relationships with significant others in our life.
Active or Passive

Attachment patterns are strategies of communicating with a caregiver, and the ability to use that caregiver to become calm when faced with stress. Avoidant children have learned not to call their parent, as calls have not been attended to, or they have learned to inhibit their calls, having determined it is best not to burden their caregiver unless it is very necessary. Ambivalent children have learned to turn up the volume of their protests when distressed. They demand the presence of the caregiver loudly, and have determined that this is the best strategy for getting their needs met. In the end we have extremes of active versus passive strategies. Disorganized children may flip flop between these strategies, at times seizing control, and other times becoming passive. It is important to point out here that the child’s behavior is not related to the parents love for their child. Parents who very much love their children can be unavailable for many reasons or can be stressed by a multitude of factors. Also genetic or environmental (toxins/medical/trauma) factors may interfere with a parent's capacity to soothe a child despite their best efforts and availability. Any one of these strategies may be a functional strategy in such situations for a child.
In the last post we explored how children learn to accommodate their behaviour to the needs of others. In this post we have seen how children communicate responsibility to those others for their needs. These relationship patterns persist into adulthood and determine the patterns we engage in, in our most intimate relationships, when we are in need. These intimate relationships in turn are the relationships we rely on for support when we become the caregivers for the next generation. We, as a society, are charged with providing as supportive a community as possible to young parents, of all attachment styles, as they face the challenges of meeting the needs of their young ones. In this way we allow them the best opportunity to create sustaining relationships that will provide a strong foundation for the next generation.
Sunday, 21 October 2012
Putting on the Brakes
In my last post I reviewed the first nine months of human development. In this post I will review the next nine months. Both genetics and early relationships have something to do with how our moods change through our lifetime and these second nine months can be critical to how this goes.
Parents Say No

There is a profound change that occurs in the relationship between an infant and its mother in this next time period. This change has implications for shaping the person that we will become. The first nine months can involve a lot of warm and fuzzy interactions between mother and infant. Laughing and cooing and cuddling. During the first nine months the child’s capacity for tolerating the world of the senses and ideally the capacity to enjoy human contact and exploration develops. The next nine months take on a different dynamic between parent and infant, a change that happens in even the most successful relationships. As the child becomes more mobile the parent takes on the role of supervisor and parent directions towards the child skyrocket compared to the first period. “Don’t touch that.” “Don’t go there.” “Don’t put that in your mouth.” You get the picture. Infants don’t learn to say “no” at this time, that comes later, but parents start to say “No”, a lot.
Those Eyes

During these next nine months the growth burst in connections in the right brain continues. According to Allan Schore there is a new pathway being laid down during this period. During this time the infant may, or may not, develop the ability to put the brakes on their exploration of the world. As in the first period, the brain develops connections between the planning parts of the brain (frontal cortex) and the emotional brain that controls our physical state (limbic system). The connections that may develop now allow the child to stop certain socially undesirable or possibly unsafe behaviours. The infant is now mobile enough to move away from the parent but will pause from time to time to look to the parent for those flashing, approving eyes. But if, for example, they have drawn a masterpiece on the living room wall, they might receive a different look. Those eyes will reflect disapproval, maybe even anger.
Shame and Repair

The “parasympathetic” reaction that follows will lead the child to become deflated. The eyes drop, the heart rate and motor output slows, and the child has had his first experience of shame. The infant of course, does not identify this emotion. Identifying emotions is a left brain task, which doesn’t develop until later (if it develops at all). This interaction, when it goes well, can have the happy result of the child learning that drawing on the wall is not acceptable. Shame, although much maligned, is part of normal healthy development. The key part of this interaction being adaptive, comes with the next part of the interaction. The stage that may hopefully follows, is the stage of repair. The child reconnects with the parent tentatively and gradually, and the positive relationship is re-initiated. When these two steps are successfully repeated over hundreds of interactions, a new type of regulation is achieved. The regulation of high energy, active, exploratory, mood states and low energy, quiescent, reflective mood states. The ability to tolerate frustration and even failure has its origins here, as does the ability to take responsibility when faced with expectations from others. These can be difficult waters to navigate. The infantile temper tantrum can emerge at this time, when children have difficulty making the transition from one mood state to the next. This, of course, has the potential to increase the stress level of the parent who will require considerable support, him or herself, to stay regulated in the face of flying food or cutlery.
Two roads

Interestingly, we can see the development of two patterns emerging in this second stage. As mentioned last time, infants can be identified at birth (even prenatally) as high sensitivity and low sensitivity infants, with an average group in between. Jerome Kagan famously followed groups of children through childhood and determined that high sensitivity infants were likely to become inhibited children and low sensitivity infants tended to become uninhibited children. Parental influences did make a difference as far as avoiding the extremes of recklessness for uninhibited children and high anxiety for inhibited children, but Kagan noted that high sensitivity children almost never became very daring and low sensitivity children almost never became highly cautious.
Tigger vs Eeyore

By the time this second developmental period is over, children will have developed a consistent pattern of mood states which form their emerging character. Much like the characters from the children’s story Winnie the Pooh, some will bounce along in persistent high energy states, rather impervious to direction, much like Tigger. Others will spend much of their time in highly anxious mood states, sensitive to direction, much like Piglet. Still others will reside in chronic low energy, high shame, mood states like Eeyore. And still others will lurch dramatically between mood states, more like Jeckyl and Hyde. Ideally there will be smooth and flexible mood states. With flexibility, comes the ability to take responsibility for one’s actions and tolerate responsibility, frustration and even failure while not feeling crushed by these experiences. What is critical to understand is that the relationship is at the center of this development. It is in the relationship that the ability to regulate sensation (last post) develops and it is in the relationship that the ability to regulate mood states develops. Biological factors can make the difference between children who are likely to overreact, and those that are likely to underreact, but these patterns will develop in the relationship and, with support, relationships can lead the way to new abilities which may develop at any time in the lifespan.
Sunday, 14 October 2012
Keeping it Regulated
In the next series of posts I want to walk you through the complex process of human development as we understand it.







In the first nine months of life the basic ability to regulate stimulation is beginning to develop. Allan Schore, in his series of texts, has compiled vast amounts of interdisciplinary research tracking the neural pathways in the right hemisphere that link our sensory brain to our planning brain and relay directly to our limbic system (emotional, physical control centres) that encode these mind-body interactions which we refer to as sensory-emotional regulation. Do you shy away from busy situations or do you seek them out? Do you detest quiet setting or do you thrive in them? This dance of genetic potential with environmental feedback in these nine months has a lot to do with it. Remember however that mother alone is not responsible for what happens here. Mothers themselves (as you might remember from my last post) are not islands. Their own stress levels are dependent on those around them. The support of fathers, extended family and the broader community has everything to do with the stress level under which any mother will be operating both during pregnancy and thereafter. Our society as a whole has responsibility for how stressful an environment these early years will be.
Who are we?
The debate whether we begin our lives as a “tabula rasa” (blank slate) verses having our development predestined, be it from God or from genetics is an ancient one. In addition to this, I want to explore the question of how much we can know about who we are. You may have heard of Renee Descartes, a philosopher who famously said "I think therefore I am", ushering in an era of human rationality known as the Enlightenment. Descartes was referring to the amazing ability we humans have for conscious reflection. Certainly this amazing ability is a powerful tool, but modern neuroscience increasingly reveals that, in fact, it represents only a relatively small proportion of who we are.
Our study of human development has revealed that an amazing amount of neural development occurs in bursts over the first three years of human life (including prenatally), well before we are capable of conscious reflection. Here we may begin to explore the evolution of some of the layers of who we are, as they are laid down in a complex dance of inborn potential and environmental feedback.
The Brain

Neural development, of course, involves all the major structures of the brain, however development appears to occur earlier for certain structures than others. Interestingly, it is the right hemisphere that appears to develop earliest. You may know that we humans have an interestingly divided neurology. We have a cerebral cortex, that highest level layer of our brain, that is divided in two, joined by a remarkably narrow strip of brain matter known as the corpus callosum. Each side of the brain is preferentially connected to the opposite side of the body, but these two hemispheres have also been shown to have very different ways of processing our lived world. A recent work by Iain McGilchrist (The Master and his Emissary) does a comprehensive job of illustrating the implications of this lateralization of human consciousness.
This earlier developing right hemisphere certainly learns, and it certainly thinks, but it's learning and thinking happen implicitly. That is, learning happens through experience and is recalled automatically and unconsciously, leading to changes in our physical states including our emotional states. In human infants the learning and development that occurs first are various forms of bodily and sensory regulation. As you may know from experience, tiny infants cannot yet regulate almost anything about themselves. Unlike some creatures, who can be independent even at birth, humans have some of the most dependent infants in the animal kingdom. Human infants require the constant presence of the caregiver for regulation, and as studies of Romanian orphans have shown, the implications of having little physical contact with a caregiver, even in the presence of adequate food, water and shelter are profound and often devastating. Our emerging genetic potential requires the scaffolding of a human relationship to unfold from the very beginning.
Nature and Nurture

Michael Meaney is a Canadian researcher who has done some fascinating work in the implications of infant mother interactions and the implications for this for gene expression. The word for environmental experiences that influence gene expression is “epigenetics”, and our understanding of this process is only just beginning. These very early interactions appear to be fundamental in the expression of certain genes that have major implications for behaviour and stress reactivity. In rats, the parental behaviour that triggers gene expression is anogenital licking. In humans it is a series of interactions that lay the groundwork for our ability to navigate the sensory and interpersonal world that we will be living in.
Pregnancy

Even prenatal development involves more than simple genetic unfolding. We know that stress during pregnancy increases the risk for premature birth and low birth weight, which are associated with various adverse health and developmental outcomes. Some recent studies have suggested increased rates of ADHD, anxiety and mood disorders, although this is a surprisingly under-researched area. Temperament may also be affected with infants whose mothers have been highly stressed showing temperaments at the extreme ends of the spectrum. It seems that genetics does contribute significantly to temperament at birth, determining how an infant may respond to stress, with either increased or decreased reactivity to stimulation.
The Dance

The first nine months or so of human development involve an incredible surge of brain development. The senses of smell and touch are most important initially, when physical contact are paramount. Vision and hearing then play an increasing role. Here our preoccupation with the human face and voice begin. In particular, the eyes. Babies seek out the face of the mother and an incredible conversation begins. A conversation held with caresses, flashing eyes and playful vocalizations. In this interaction the baby develops an increasing ability and even enthusiasm for processing information. The mother is the guardian of stimulation. It is her job to optimize the amount of stimulation, much of it which will be coming from her. A "three bears" rule of not too little, not too much rule is something the baby manages on his end by seeking, calling and looking away. The mother intuitively responds to these cues from her end. The match between the mothers natural inclination to stimulate, her stress level, and the infants partially genetically determined optimal window of stimulation seems to be key here. This is what some researchers have referred to as “goodness of fit”. This window is a sensitive one and as we know from "Still face" experiments, a period of rupture from this dance of interaction can be very distressing for the infant, who as yet cannot navigate this world of stimulation.
Orchids and Dandelions

Some genetics appear to allow children to develop well enough in a wide range of environments while other genetics lead to high sensitivity which appears to lead to very good outcomes in well matched environments but very poor outcomes in other environments. Bruce Ellis, a family researcher at University of Arizona, coined the term “orchid children” to refer to these highly sensitive children with the more fragile genetic make-up. He referred to the hardier children as “dandelion children".
Introverts and Extroverts

In the first nine months of life the basic ability to regulate stimulation is beginning to develop. Allan Schore, in his series of texts, has compiled vast amounts of interdisciplinary research tracking the neural pathways in the right hemisphere that link our sensory brain to our planning brain and relay directly to our limbic system (emotional, physical control centres) that encode these mind-body interactions which we refer to as sensory-emotional regulation. Do you shy away from busy situations or do you seek them out? Do you detest quiet setting or do you thrive in them? This dance of genetic potential with environmental feedback in these nine months has a lot to do with it. Remember however that mother alone is not responsible for what happens here. Mothers themselves (as you might remember from my last post) are not islands. Their own stress levels are dependent on those around them. The support of fathers, extended family and the broader community has everything to do with the stress level under which any mother will be operating both during pregnancy and thereafter. Our society as a whole has responsibility for how stressful an environment these early years will be.
Change is possible
The amazing thing about development is that although there are important windows, the story if never fully determined. New developments can always emerge and neuroplasticity for change is much greater than we once believed. In the next few posts I will cover some of the next milestones the human infant will cross as we travel this complicated terrain of human development.
Sunday, 7 October 2012
Mothers and Others
In the next few posts I want to explore human development from a few different angles. In the current post I want to look at evolutionary and cultural factors. Relatively recent findings have helped us gain a greater understanding of how human development is influenced by its relational context. Laboratory studies bring us useful information about development, however human development does not occur in a Skinner box or a test tube. By the same principles any change we undergo at any point in our development will also occur in a relational context.

Not just another Ape
I have borrowed the title for this post from the title of a groundbreaking book by Sarah Hrdy (2009) an accomplished anthropologist . In this book, Hrdy takes us on a journey across genetics, cultures and time to get to know our species and our unique way of raising offspring. Along the way we discover some fascinating truths about who we are. Due to our physical attributes (bipedal, big headedness), we humans give birth to our young at a very vulnerable stage Just as uniquely among primates, human mothers share the caregiving responsibilities for infants with other relatives. What you might not know, is that no other great apes or even monkeys do this (although some species of marmosets do). All other primates leave the care of the young entirely to the mother. Human mothers alone, among great apes, allow other females and even males to hold and even feed infants from the moment they are born. In hunter gatherer societies women expect the support of others in the clan, most importantly female relatives in the care of offspring. Humans throughout their evolutionary history have counted on "alloparents" for help in raising infants and this has allowed humans to have children more frequently than similar, slow developing primates. Humans tend to space children out by 2 years, whereas gorillas have offspring about 4 years apart and orangutans about 8 years apart. It is disturbing to learn that alloparenting marmosets as well as hunter gatherer humans are likely to commit infanticide when support from female relatives is unavailable. This behavior is extremely rare among other primates under similar conditions. It is not difficult to imagine the importance of determining whether an adult is a nurturing other or not for an immature member of the clan. This evolutionary situation may very well have selected for our highly developed ability to take one another’s perspective and the extension of this into language.

From Matriarchs to Patriarchs
Hrdy's last chapter offers some further thought provoking analysis from her perspective as an anthropologist. Hunter gathers developed strong tendencies to nurture one another’s offspring in order to survive, and this strategy was so successful, that many cultures came to refer to the world with various terms that approximate "the giving place". Most hunter gatherer cultures developed powerful taboos against arrogance and individualism. Mothers tended to stay with their own mothers and female kin which promoted this "alloparenting" and cooperative care. With the advent of horticulture, animal husbandry and then agriculture, surpluses of grain and livestock, and the control of property and land, things changed (from about 10 000 years ago in central Asia to the past century in a few societies). There was now property and land to protect and thus to steal. Men began to rely on their fathers and brothers to protect these resources and mothers no longer stayed with their mothers, and often came to be seen as needing protection in a patrilineal, patriarchal social structure which eroded the nurturing matrilineal care human infants had relied on until then as well as many of the taboos mentioned above. "The giving place" was forever changed. Hrdy is not alone in hypothesizing that this shift marked a significant change in the history of childhood and childcare that has had tremendous repercussions.

The Modern World

An afterthought… I don't mean to come across as all “noble savage”. Hunter gatherer life was hard, and lifespans were short. The modern world has unleashed amazing creative potential in science, arts and medicine. I don't propose a retreat from modernity. What I propose is applying ourselves to understanding our modern ills holistically, so that we can find a way to apply this amazing creative potential to modern solutions.
Tuesday, 2 October 2012
Collaboration vs Behaviour Modification
One of the earliest decisions we made on the Adolescent Psychiatric Unit was a decision on what approach we would take towards the behaviour of young people on our ward.
As you may know psychiatry has gone through phases over its history. From the outset there have been two dominant schools of thought in terms of mental illness. A moral model which sees mental illness as a moral or spiritual problem and a medical model which sees mental illness as a disease of the brain. Both of these competing models still exist in various form today. (More on this in future posts.) The turn of the century saw the dawning of the psychoanalytic model which framed mental illness as "conflict" between conscious and unconscious processes, where unconscious drives overwhelmed the conscious mind leading to various symptoms of illness. As the century progressed a new paradigm took centre stage. Behaviourism arrived with the discipline of research based psychology. Behaviourism developed models of learning and behaviour that could be measured for research purposes, and dismissed motivational and emotional states that were more difficult to measure. Both of these models were fruitful in different ways but also led down sometimes unhelpful roads. Unhelpful interpretations of the psychoanalytic model such as the common understanding of Dr. Spock's advice came on the scene. This interpretation was that all we had to do was love children unconditionally and they would thrive. This unfortunately missed the fact that it is natural for us to have expectations of children and give them responsibility, which they often resist. From the behaviorists came recommendations to reward and punish and shape children's behaviour much as we would train circus animals. This misses the point that rewards and punishments only work in the context of a healthy relationship which they themselves do not help establish.
Fortunately there have been new developments in the realms of developmental science upon which we may draw. In the 1950s John Bowlby and his student Mary Ainsworth introduced Attachment Theory to our theoretical repetoire. Borrowing from ethology, these clinicians used observational methods to establish that children develop patterns of behaviour in a relational context with their parents to establish a predictable pattern of establishing security which endure over time, generalize to relationships with significant others and romantic partners, and are often passed on from parent to child. New developments in behavioral neuroscience such as the establishment of the existence of mirror neurons and research on the process of parent child attunement have helped us gain an improved understanding of the developmental pathways for empathy and of theory of mind. These developments allow us to understand that learning occurs best in an attuned and secure relationship and at best involves more than simple conditioning.
On the Adolescent Psychiatric Unit we have followed a model of "Collaborative Problem Solving" (with start up consultation from Ross Greene). What we have moved away from is the model of Behaviour Modification which still dominates on many, perhaps most, hospital wards. In the Behaviour Modification model rewards are given for desirable behaviour and consequences meted out for undesirable behaviour. The problem with the behaviour modification model is that those who can cope with it are rewarded while those who can't are punished. What you get in the end is extremes of behaviour. Studies have shown that these kinds of interventions increase the rates of seclusion and restraint. Collaboration involves having and discussing expectations while taking the time to listen to the concerns and expectations of the young person. It involves understanding that young people may not always be able to meet our expectations, but that there are many different reasons why they may not. Using this model we can learn what some of the barriers to meeting the expectations of others might be in this particular child, increasing our understanding, while improving communication skills and trust. In a relationship where kids feel safe and understood they usually come to accept the expectations of others. So far this model has worked well for us, although it can be challenging and requires more thoughtfulness and effort than a simple behavioral model would require. Overall the results have been rewarding and our restraint and seclusion rates have been near non-existant.
As you may know psychiatry has gone through phases over its history. From the outset there have been two dominant schools of thought in terms of mental illness. A moral model which sees mental illness as a moral or spiritual problem and a medical model which sees mental illness as a disease of the brain. Both of these competing models still exist in various form today. (More on this in future posts.) The turn of the century saw the dawning of the psychoanalytic model which framed mental illness as "conflict" between conscious and unconscious processes, where unconscious drives overwhelmed the conscious mind leading to various symptoms of illness. As the century progressed a new paradigm took centre stage. Behaviourism arrived with the discipline of research based psychology. Behaviourism developed models of learning and behaviour that could be measured for research purposes, and dismissed motivational and emotional states that were more difficult to measure. Both of these models were fruitful in different ways but also led down sometimes unhelpful roads. Unhelpful interpretations of the psychoanalytic model such as the common understanding of Dr. Spock's advice came on the scene. This interpretation was that all we had to do was love children unconditionally and they would thrive. This unfortunately missed the fact that it is natural for us to have expectations of children and give them responsibility, which they often resist. From the behaviorists came recommendations to reward and punish and shape children's behaviour much as we would train circus animals. This misses the point that rewards and punishments only work in the context of a healthy relationship which they themselves do not help establish.
Fortunately there have been new developments in the realms of developmental science upon which we may draw. In the 1950s John Bowlby and his student Mary Ainsworth introduced Attachment Theory to our theoretical repetoire. Borrowing from ethology, these clinicians used observational methods to establish that children develop patterns of behaviour in a relational context with their parents to establish a predictable pattern of establishing security which endure over time, generalize to relationships with significant others and romantic partners, and are often passed on from parent to child. New developments in behavioral neuroscience such as the establishment of the existence of mirror neurons and research on the process of parent child attunement have helped us gain an improved understanding of the developmental pathways for empathy and of theory of mind. These developments allow us to understand that learning occurs best in an attuned and secure relationship and at best involves more than simple conditioning.
On the Adolescent Psychiatric Unit we have followed a model of "Collaborative Problem Solving" (with start up consultation from Ross Greene). What we have moved away from is the model of Behaviour Modification which still dominates on many, perhaps most, hospital wards. In the Behaviour Modification model rewards are given for desirable behaviour and consequences meted out for undesirable behaviour. The problem with the behaviour modification model is that those who can cope with it are rewarded while those who can't are punished. What you get in the end is extremes of behaviour. Studies have shown that these kinds of interventions increase the rates of seclusion and restraint. Collaboration involves having and discussing expectations while taking the time to listen to the concerns and expectations of the young person. It involves understanding that young people may not always be able to meet our expectations, but that there are many different reasons why they may not. Using this model we can learn what some of the barriers to meeting the expectations of others might be in this particular child, increasing our understanding, while improving communication skills and trust. In a relationship where kids feel safe and understood they usually come to accept the expectations of others. So far this model has worked well for us, although it can be challenging and requires more thoughtfulness and effort than a simple behavioral model would require. Overall the results have been rewarding and our restraint and seclusion rates have been near non-existant.
Introduction
I envision this blog as a way to reach out to other people working in the field of Youth Mental Health, or struggling with issues that relate to the mental health of young people.
I am a Psychiatrist working on a specialized hospital unit for young people struggling with mental health issues in Kelowna, British Columbia, Canada. I also work on call at this hospital and am consulted to support young people in crisis in the Emergency Department and on the Paediatric Ward.
As you can imagine this kind of work forces one to confront some challenging ethical questions as well as some important theoretical questions, such as:
What exactly is mental illness?
What aspects of treatment should young people decide for themselves, how does this change with development?
What aspects of treatment should people with mental illness decide for themselves?
What is the role of family in these decisions?
How do we address the behaviours of young people, or mentally ill people in the hospital?
How do families address the behaviours of young people, including those with mental illness at home and how is this the same or different?
What is the role of medication in treating young people?
What is the role of various other treatments in the hospital and after hospital in treating young people?
I see this blog as being a forum for discussion on these topics. My team here on the Adolescent Psychitric Unit have wrestled and continue to wrestle with these questions and I will share some of our philosphical postitions on these matters in this blog as well as the role of various advances in the realm of developmental science and neuroscience that might inform these questions.
I am a Psychiatrist working on a specialized hospital unit for young people struggling with mental health issues in Kelowna, British Columbia, Canada. I also work on call at this hospital and am consulted to support young people in crisis in the Emergency Department and on the Paediatric Ward.
As you can imagine this kind of work forces one to confront some challenging ethical questions as well as some important theoretical questions, such as:
What exactly is mental illness?
What aspects of treatment should young people decide for themselves, how does this change with development?
What aspects of treatment should people with mental illness decide for themselves?
What is the role of family in these decisions?
How do we address the behaviours of young people, or mentally ill people in the hospital?
How do families address the behaviours of young people, including those with mental illness at home and how is this the same or different?
What is the role of medication in treating young people?
What is the role of various other treatments in the hospital and after hospital in treating young people?
I see this blog as being a forum for discussion on these topics. My team here on the Adolescent Psychitric Unit have wrestled and continue to wrestle with these questions and I will share some of our philosphical postitions on these matters in this blog as well as the role of various advances in the realm of developmental science and neuroscience that might inform these questions.
Subscribe to:
Comments (Atom)